
Welcome to the Center for Comprehensive Breast Care
Since 1995
At the Comprehensive Center for Breast Care at ASBS, we are dedicated to providing the highest quality of care to patients diagnosed with breast cancer. Our Center brings together the South Bay’s premier multidisciplinary breast cancer team. Specialists from medical, radiation, and surgical oncology work together to provide the most advanced individualized treatment plans. We treat close to 500 women each year and offer comprehensive screening, diagnostic, medical and surgical breast services, nutrition and genetics counseling, and a full array of psycho-social support for patients and families.
Our breast surgeons coordinate complex treatment planning with all team members, providing a comprehensive, multidisciplinary approach to benign and malignant diseases of the breast, and collaborating closely with other specialists at the Torrance Memorial Breast Diagnostic Center and the Providence Little Company of Mary Torrance Women’s Imaging Center.
Our breast surgeons work closely with their patients to identify a surgical option that provides for the best outcome taking personal concerns and preferences into consideration. Some options include:
- Oncoplastic surgical techniques for better outcomes
- Skin sparing or nipple sparing mastectomy
- Sentinel lymph node biopsy and selective axillary node dissection
- Immediate reconstruction in coordination with plastic surgeons
- Surgical treatment for high risk or BRCA mutation carriers
Our Breast Center Team

James E. Camel
MD, MS, FACS
Robotic & General Surgery

Melanie H. Friedlander
MD, FACS
Breast & General Surgery & Minimally Invasive Surgery

Catherine A. Madorin
MD, FACS
Endocrine & General Surgery
James E. Camel
MD, MS, FACS
Robotic & General Surgery

Son Nguyen
MD, FACS, Director
Skin Cancer, Hernia, & Colorectal Surgery

Albert Y. Lam
MD, FACS, Director
Skin Cancer, Hernia, & General Surgery
Breast Cancer 101

- Breast cancer is the most common cancer in American women > 200,000 females diagnosed with breast cancer per year
- It is the second most common cause of cancer death in women
- It’s the number one cause of death in females age 45-55
- Abnormal cells develop from normal cells in the breast to form tumors
- Tumor cells have genetic defects that allow the cells to grow too rapidly and to invade normal tissues
- 90% of women with breast cancer have tumors due to spontaneous new mutations arising in their breast tissue as they age
- Direct extension
- Lymphatic spread
- Hematogenous spread

Most breast cancer patients undergo surgery to remove cancer from the breast. The majority of women are candidates for breast conserving surgery, commonly referred to as lumpectomy, which involves removing the portion of breast containing the tumor along with an adequate amount of normal breast tissue.
A quadrantectomy is a type of breast-conserving surgery more commonly performed in Europe than in the U.S. This surgery involves removal of a fourth of the breast tissue in an effort to reduce the need for re-excision and potentially the risk of recurrence. The downside of this method is that a patient is often left with a large defect without a significant benefit over lumpectomy.
While most patients are candidates for breast conserving therapy, and the majority of women elect this method, some patients are appropriate candidates for mastectomy, or the removal of the entire breast. Some additional tissue, such as lymph nodes from the underarm, may need to be removed as well.
A patient should consider a mastectomy in the following cases: 
- Cancer that extends to another quadrant of her breast
- Malignant cells present in multiple quadrants of her breast
- Very large tumors
- A tumor that does either does not shrink while on pre-operative chemotherapy
- A history of radiation treatment
- The inability to undergo radiation treatment (for example, because of pregnancy)
- Not all mastectomies are created equal: there are many different kinds of mastectomies available to patients. And often times, it is both safe and preferable to perform breast reconstruction in the same setting, i.e. immediately following the mastectomy operation, while a patient is still under anesthesia. Reconstructive options can either be implant-based or take advantage of a patient’s own tissue (See http://www.diepflap.com)
Simple (total) Mastectomy:
This operation involves the removal of all breast tissue. Often, the lymph nodes from under the arm will be sampled (sentinel node biopsy) but not removed. This operation can be undertaken via a skin-sparing approach (see below) or in a more traditional fashion, removing the skin overlying the breast.
Modified Radical Mastectomy:
The modified radical mastectomy removes all tissue of the breast, including the fascia, or casing, of the pectoralis muscle, as well as removal of some (not all) of the axillary (underarm) lymph nodes. The pectoralis muscles are not removed in this operation.
Radical Mastectomy:
This procedure, first introduced over a century ago, involves radical removal of underarm lymph nodes, removal of the pectoralis muscles, in addition to the breast gland. Because of increased understanding and research on the nature of tumors, radical mastrctomy is rarely undertaken today. It is reserved for patients with locally advanced tumor invading the chest wall.


- Female gender
- Increasing age
- Family history
- Early menarche/Late menopause
- Older age at 1st live birth
- Prolonged HRT
- Benign proliferative breast disease
- Genetic mutations
Surgery
Association Of South Bay Surgeons Contents Specialties South Bay Breast Center Surgery
Once diagnosed with breast cancer it is essential to educate yourself about treatment options. Meeting with an experienced breast surgeon is important.
At the Center for Comprehensive Breast Care, your breast surgeon will consider a number of factors in order to provide the best surgical plan. These factors include:
- The size of the breast cancer
- The characteristics of the breast cancer tumor(s)
- The location of the tumor(s) within the breast
- The breast size of the patient
- The presence of enlarged or suspicious axillary lymph nodes
- Each patients unique psychosocial circumstances and factors including, quality of life issues, long-term peace of mind, emotional well-being.
Lumpectomies
- Removes only the tumor and a small rim of normal tissue around it.
- Preserves the shape and contour of the breast.
- If a breast cancer is not palpable, a wire may be placed preoperatively to help the surgeon determine which portion of breast tissue to remove.
- May require additional surgery if the 1st lumpectomy tissue had positive margins (cancer extending to the edge).
Mastectomies
Surgical removal of the entire breast.
Types of mastectomy:
- Total (simple)
- Modified radical
- Skin sparing
- Prophylactic
Skin sparing mastectomies and reconstruction
Popular alternative to traditional mastectomy for treatment and prevention of breast cancer in selected patients.
Involves removal of the breast gland with preservation of the native overlying skin.
Generally results in smaller, less obvious scars, and preservation of the patient’s native skin envelop which can then be used to reconstruct the breast.
Skin and nipple sparing mastectomies are becoming a popular alternative to traditional mastectomy for both treatment and prevention of breast cancer. The skin sparing mastectomy involves removal of the breast gland with preservation of the native skin overlying the breast. This generally results in smaller, less obvious scars, and preservation of a patient’s native skin envelope, which can then be used to reconstruct the breast, maintaining and sometimes improving the natural shape and contour of the breast. The reconstruction portion of the surgery is performed by a plastic surgeon. Typically, the reconstruction is performed in a staged manner.
The nipple-sparing variant of a skin-sparing mastectomy leave the patient’s own nipple and areola behind in order to maximize the natural look of a patient’s breast. Not everyone is a candidate for the nipple-sparing mastectomy, but your surgeon will work with you to decide what’s right for you.
Nipple-sparing mastectomy has not been compared to traditional mastectomy or standard skin-sparing mastectomy in head-to-head trials. However, our current retrospective data reflects the relative oncologic safety of the procedure.
Sentinel Lymph Node Mapping and Biopsy
In order to see if the breast cancer has spread to the lymph nodes, a biopsy of the nearest lymph nodes is performed. The sentinel lymph node biopsy is an improvement on traditional axillary lymph node dissection, requiring far fewer lymph nodes to be removed than in the past. Lymph nodes in the armpit are sequentially aligned, if breast cancer cells are not discovered in the first (or sentinel) lymph nodes, then there is no need to dissect the subsequent ones. This helps avoid the removal of several lymph nodes under the armpit, a procedure known to cause unpleasant problems such as lymphedema (arm swelling).
Either on the day prior or day of breast cancer surgery, a physician or technician will inject a radioactive material into the breast to help locate the sentinel node. In the operating room the surgeon may also inject a blue dye as a second method of finding the sentinel node. Usually, 1-3 nodes contain either blue dye, radioactivity, or both. All such nodes must be removed and evaluated by the pathologist. This is generally done through a small incision hidden in a crease in the armpit. If no cancer cells are present, it can be assumed with over 90% certainty that there are no cancer cells present in any of the underarm nodes.
Axillary Lymph Node Dissections
An axillary dissection is performed if a patient has a positive sentinel lymph node biopsy or palpable axilla lymph nodes that contain cancer on a preoperative biopsy. An axillary lymph nodes dissection is performed via an underarm incision and removes the area of fatty tissue in the armpit. This area of fatty tissue usually contains 10-20 lymph nodes. The tissue is sent to the pathologist and evaluated to determine the total number of lymph nodes and the number positive for cancer. This information will be used to determine your cancer stage and possible further treatment.
Brachytherapy Catheters
Radiation therapy commonly is used after lumpectomy to treat early-stage breast cancer and reduce the risk of the cancer coming back (recurrence). Brachytherapy is a newer form of radiation therapy and an alternative to traditional whole-breast external beam radiation therapy for a select group of patients. Brachytherapy delivers a higher dose of radiation to a smaller area of the breast over a shorter period of time compared to traditional (external beam) radiation therapy. Doctors sometimes refer to brachytherapy as accelerated partial breast irradiation (APBI).
This approach requires the placement of a special tube with a balloon on one end in the breast where the cancer was. The tube comes out of the skin through a small hole. The tube and balloon are placed after lumpectomy surgery in a surgeon’s office. During each treatment, a machine places a radioactive seed into the center of the balloon for 5 to 10 minutes — just long enough to deliver the required dose of radiation. After the seed is removed, you may leave the treatment center. A total of 10 treatments are usually given over 5 days. That means two treatments per day, about 6 hours apart. When the final treatment is done, the balloon and tube are removed through the small hole in the skin.
Portacatheter Placements
Portacatheters are long, narrow, hollow tubes made of soft plastic that are often used to deliver chemotherapy. These catheters are placed completely under the skin and connected to a small plastic or metal disc called a port. During treatment, the port is accessed by an IV needle to infuse chemotherapeutic medication into the vein. Patients requiring long term chemotherapy may benefit for portacatheters as they spare the need for repeated peripheral IV placement.
Sentinel Lymph Node mapping in Melanoma and Breast Cancer
Association Of South Bay Surgeons Contents Specialties South Bay Breast Center Lymph Node Surgery
Like many cancers, malignant melanoma and invasive breast cancer often spread from their original site through the lymph channels to regional lymph nodes. With melanoma, removal of these lymph nodes can prolong life and in some cases cure the disease; in breast cancer removal of these lymph nodes provides prognostic information regarding cure and can help decide whether there is a need for chemotherapy.
There clearly appears to be a role for the removal of regional lymph nodes in melanoma and invasive breast cancer. Unfortunately, this operation is often leads to a significant number of temporary and permanent complications including arm and leg swelling, poorly healing incisions and a loss of skin sensation. When the regional lymph nodes are removed in intermediate depth melanoma less than 15 percent of patients have proven metastasis(i.e., cancer in the lymph nodes), while less than 20 percent of patients with early breast cancer have proven metastasis. The routine use of lymph node removal in these two cancers unnecessarily exposes all these patients to the complications of the procedure while providing benefit to only those with metastatic disease.
Sentinel lymph node mapping is a new way to evaluate regional lymph nodes. It is currently in routine use for the treatment of malignant melanoma and is under study for its role in breast cancer. This minimal surgical procedure spares 80 percent of patients the greater surgical procedure of regional lymph node dissection by identifying those patients that will benefit from the more extensive removal of lymph nodes. This approach allows the surgeon to identify and biopsy the first or “sentinel” lymph node which the cancer encounters as it spreads to the regional lymph nodes. If the sentinel lymph node is free of cancer, studies show that all lymph nodes in that region are free of cancer and complete lymph node removal is unnecessary.
Two hours before the operation the radiologist injects a nuclear isotope around the melanoma or breast cancer and 45 minutes later obtains a nuclear scan to determine the “hot” sentinel lymph nodes to which the isotope has spread. Fifteen minutes before the operation begins, the surgeon injects a blue vegetable dye around the tumor site which also helps identify the lymph nodes. In the operating room, the melanoma or breast cancer is excised first and then the sentinel lymph node is identified. Using a hand-held Geiger counter, the surgeon pinpoints the sentinel lymph nodes beneath the skin and makes a small incision over them. Using the Geiger counter and visualizing the blue dye which has spread to the sentinel lymph nodes, the surgeon can isolate and remove these with minimal dissection. This completes the surgery and only if subsequent studies demonstrate metastatic tumor in the sentinel lymph nodes will complete lymph node removal be recommended Preoperative lymph node mapping and lymph node biopsy (removal) and combined with wide excision of the local melanoma or breast cancer will often be the only surgical procedure required.
At the present time we are able to offer this procedure at Torrance Memorial Medical Center and at Little Company of Mary Hospital. While some surgeons use the isotope or blue dye alone, we believe the two in combination offer the greatest accuracy. We agree with most national experts that sentinel lymph node mapping is the standard of care for intermediate thickness melanomas while its role in breast cancer is still under investigation.
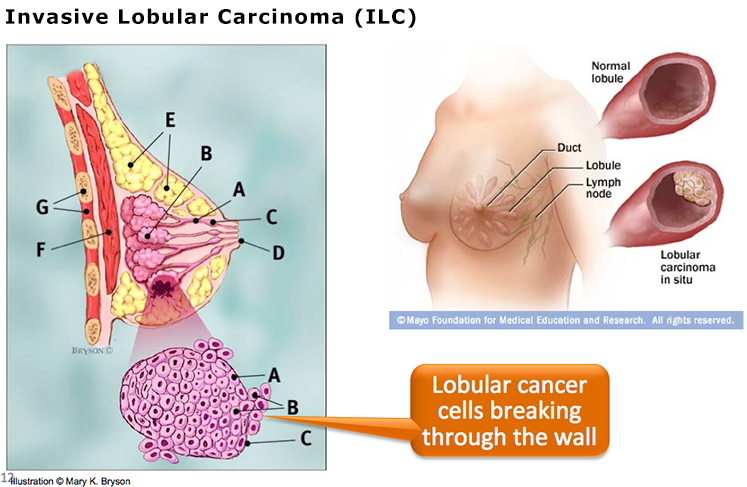
Breast Profile
- Ducts
- Lobules
- Dilated section of duct to hold milk
- Nipple
- Fat
- Pectoralis major muscle
- Chest wall/rib cage
Enlargement
- Normal duct cells
- Basement membrane (duct wall)
- Lumen (center of duct)
Lymphatic System
- Lymphatics drain fluid that carries WBCs from the breast tissues into lymph nodes in the axilla and substernal region.
- Lymph nodes filter bacteria and play a key role in fighting off infection.
Ducts
- Breast Gland
- Each breast has 15 to 20 lobes arranged like the petals of daisy.
- Inside each lobe are many smaller structures called lobules.
- At the end of each lobule are tiny sacs that can produce milk.